When you have keratoconus, your cornea undergoes gradual and progressive thinning. As the cornea thins, its shape changes.
Normally, the cornea is shaped like a rounded dome, a quality that’s essential to properly focus light, so you have a clear vision. As it thins, the middle of the cornea starts to bulge outward, forming a cone-like shape.
Keratoconus typically begins in adolescence and progressively worsens through your mid-30s before the thinning slows down or stops. But it progresses at a rate that varies for each patient.
As the disease worsens, so does your vision. Although glasses correct your vision in the early stages of keratoconus, the disease can progress to the point where eyeglasses or contact lenses no longer help.
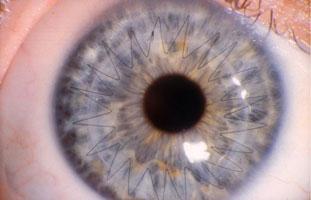
Corneal cross-linking (CXL) is a medical procedure that is used to treat certain eye conditions, particularly keratoconus and corneal ectasia. These conditions involve a thinning and weakening of the cornea, the clear, dome-shaped surface that covers the front of the eye, leading to progressive visual distortion, and reduced quality of vision.
CXL works by increasing the strength and stability of the cornea through the use of a photosensitizing agent and ultraviolet light. During the procedure, the patient receives eye drops containing riboflavin, a type of vitamin B2, which helps to absorb the ultraviolet light. The cornea is then exposed to ultraviolet A (UVA) light, which activates the riboflavin, causing the corneal collagen fibers to cross-link and become stiffer.
The strengthening effect of CXL can help to slow or even stop the progression of keratoconus and corneal ectasia, preserving the patient’s vision and reducing the need for more invasive treatments such as corneal transplants.
There are a few reasons you may not qualify for corneal cross-linking. These contraindications include:
1909 Beach Blvd #101
Jacksonville Beach, FL 32250
7205 Bentley Rd
Jacksonville, FL 32256
12341 Yellow Bluff Rd #4
Jacksonville, FL 32226
206 Ashourian Ave. #215
St. Johns, FL 32092
3 Shircliff Way Suite #134
Jacksonville FL 32204